
Chronic kidney disease is usually managed as a slow, one-directional decline. The conversation often centers on how quickly GFR is falling, when dialysis may become necessary, and whether transplant will eventually enter the picture. What is rarely discussed is the biological terrain behind that decline: the inflammatory, metabolic, vascular, and extracellular matrix conditions that may be contributing to progressive loss of kidney function in the first place.
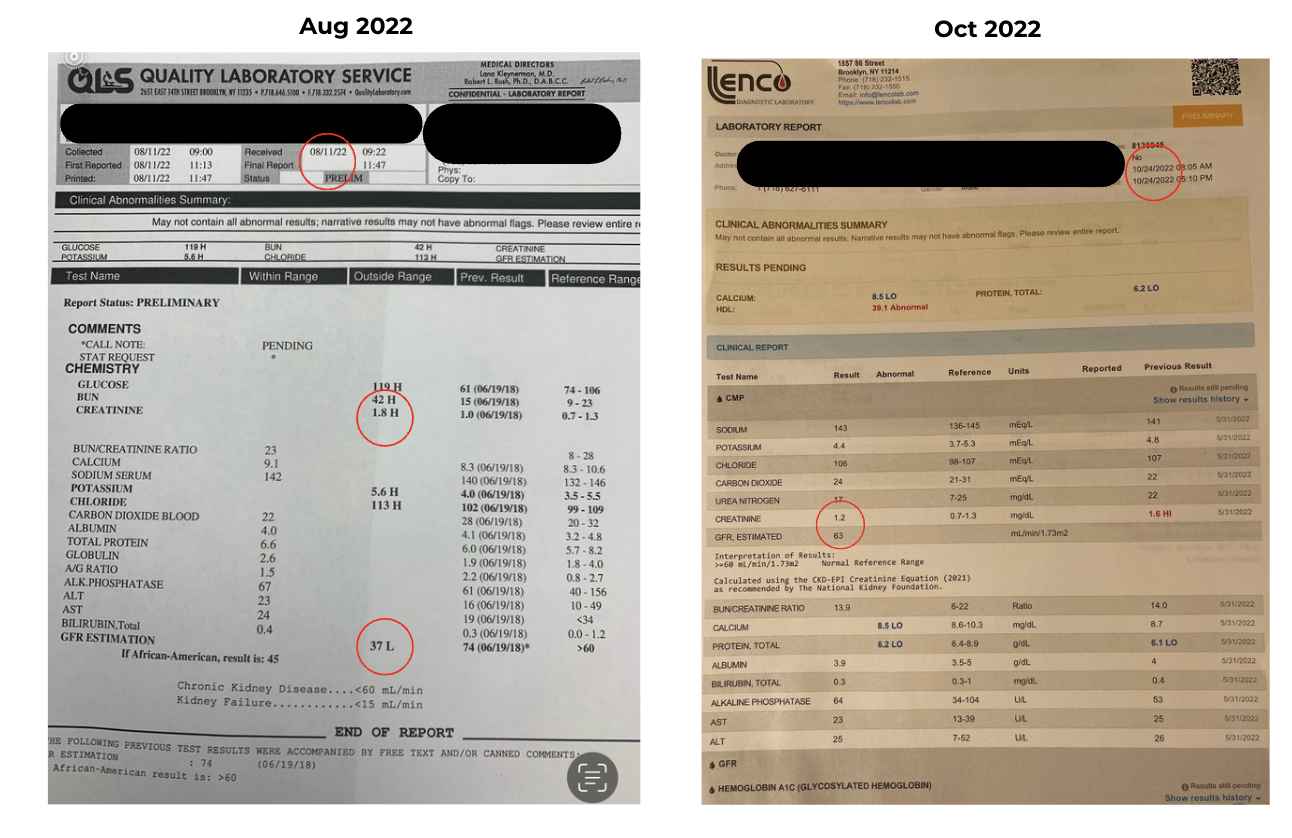
This case documents a measurable reversal of CKD progression in a 73-year-old male using European Biological Medicine drainage therapy, matrix alkalinization, and trace mineral support. GFR rose from 37 to 63 mL/min/1.73m² over approximately three months. Creatinine fell from 1.8 to 1.2 mg/dL. The patient's prior trajectory had been a documented decline from a GFR of 74 in 2019 to 37 by August 2022 - a loss of nearly half his filtration capacity over three years.
Patient Profile
A 73-year-old male presented with progressing kidney disease and a stated goal of avoiding both dialysis and kidney transplant. At initial evaluation, his GFR was 37 mL/min/1.73m² (Stage 3b CKD) and serum creatinine was 1.8 mg/dL, with BUN elevated at 42. His nephrologist had recommended watchful waiting. No nephroprotective dietary, lifestyle, or pharmacological guidance had been provided.
His cardiovascular history was significant and included familial hypercholesterolemia, six cardiac stents, reduced ejection fraction, and decades of statin therapy. He was taking Entresto (sacubitril/valsartan) for cardiac support. He had no history of diabetes or hypertension. His diet was largely Northern European, though he consumed one to two glasses of wine daily. He was a former smoker, having quit at age 35.
Presenting symptoms included fatigue, lethargy, muscle aches, and depression. These symptoms were likely multifactorial, occurring in the context of declining renal function, cardiovascular disease, aging, and long-term pharmaceutical exposure.
Naturopathic Assessment: The Terrain Behind the Decline
The kidney does not fail in isolation. In the European Biological Medicine model, organ dysfunction is understood as downstream of terrain compromise - specifically, congestion and acidification of the extracellular matrix (ECM), the fluid environment through which all nutrients, oxygen, hormones, and metabolic waste must pass between blood and cells.
This patient's history represented convergent ECM loading from multiple directions:
Long-term pharmacological burden. Decades of statin therapy, cardiovascular polypharmacy, and ongoing Entresto use create sustained demand on the liver, kidneys, and lymphatics - the primary organs responsible for processing and eliminating homotoxins. When elimination capacity is chronically exceeded, the ECM accumulates metabolic waste and pharmaceutical metabolites, becomes progressively more acidic, and loses its capacity to support normal cellular signaling and microcirculation.
Hemodynamic renal stress. Reduced ejection fraction creates chronic under-perfusion of the renal vasculature. Glomerular filtration is directly dependent on adequate renal perfusion pressure. In a patient with longstanding low ejection fraction, this represents a persistent structural headwind against which the kidneys must function.
A nephrotoxic drug combination - identified retrospectively. This point deserves particular emphasis. Entresto (sacubitril/valsartan), an angiotensin receptor blocker-neprilysin inhibitor, reduces efferent arteriolar tone at the glomerulus. NSAIDs such as ibuprofen - which this patient was taking intermittently for minor pain - blunt prostaglandin-mediated afferent arteriolar vasodilation.
The combination reduces glomerular filtration pressure from both sides of the capillary bed and is a recognized cause of acute-on-chronic kidney injury. This interaction had not been identified or addressed by the patient's conventional providers, and I did not connect it during the initial treatment period. I identified it in retrospect. It is a critical piece of clinical context: GFR improvement occurred in this patient despite continued Entresto use and intermittent NSAID exposure. Removal of the NSAID burden alone would likely have produced an additional GFR benefit.
Matrix hyperacidity. The convergence of prior smoking history, chronic alcohol exposure, long-term statin use, cardiovascular disease, and advancing age produces a predictable terrain state in the homotoxicological framework: a congested, acidified ECM in which the transport function of the ground substance is impaired, metabolic waste accumulates locally, and parenchymal cells - including renal tubular cells - are progressively retoxified by their own environment. Reckeweg's six-phase model of homotoxicosis places this patient well into the deposition-to-impregnation range, where cellular function is compromised by the quality of the matrix itself.
Treatment Protocol
The initial three-month protocol - responsible for the documented GFR and creatinine changes - consisted of oral drainage remedies, alkalinization, and mineral support.
Drainage - Primary Formula
The Hevert Detox Kit served as the foundational drainage formula. Hevert drainage remedies are classical German homeopathic combination preparations designed to simultaneously support multiple emunctory organs: liver, kidney, lymph, and digestive tract. Their multi-pathway approach addresses the reality that effective terrain drainage requires opening all downstream elimination routes before mobilizing deeper toxin stores.
Drainage - Supporting Remedies (GUNA)
After one month four GUNA remedies (Italian brand) were added to broaden terrain coverage:
GUNA Matrix - targeting ECM regulation and connective tissue drainage
GUNA Deep Cleanse - systemic detoxification support
GUNA Lympho Detox - lymphatic drainage
GUNA Bowel Plus - gastrointestinal elimination pathway support
Matrix Alkalinization
Sodium bicarbonate was administered at low therapeutic doses to address matrix hyperacidity. This is both a foundational European Biological Medicine intervention for terrain correction and one with relevant conventional support: published clinical research has examined bicarbonate supplementation as a strategy to slow CKD progression by correcting chronic metabolic acidosis, which is known to accelerate tubular damage and fibrosis in kidney disease. The mechanistic rationale - reducing acid load in the ECM and supporting the body's buffering capacity - is directly consistent with the homotoxicological model of terrain correction.
Trace Mineral Complex
A trace mineral complex was included to support enzymatic function and cellular metabolism. Long-term statin use depletes CoQ10 and disrupts mitochondrial electron transport - a likely contributor to this patient's fatigue and myalgia. Mineral repletion provides cofactor support for the metabolic and detoxification processes that drainage therapy depends upon.
Phase Two: Nettle Seed Trophorestorative (Post-October 2022)
After the October 2022 labs confirmed GFR improvement, nettle seed tincture (Urtica dioica seed) was incorporated into the ongoing protocol at 20 drops twice daily.
Nettle seed occupies a distinct category from the diuretic and alterative actions of nettle leaf (Urtica urens/dioica leaf), which appears in classical homotoxicology texts for uric acid diathesis and renal drainage support. Nettle seed is used in European herbal medicine and within naturopathic clinical practice as a kidney trophorestorative - an agent considered to have specific affinity for and restorative influence on renal tissue itself. The mechanism is not fully characterized in controlled human trials, and this should be acknowledged. The clinical use is primarily derived from herbal tradition, including the work of David Winston and others working within botanical medicine.
What was observed clinically: in the subsequent treatment period, when GFR declined episodically, reintroduction of nettle seed tincture alongside the drainage protocol was consistently followed by GFR recovery within approximately one month. This pattern repeated. Full lab documentation for those subsequent time points is not available for this report, but the clinical pattern was consistent enough to be clinically instructive.
Outcomes
October 2022 repeat labs:
GFR: 63 mL/min/1.73m² - up from 37 (Stage 3b → Stage 2 CKD)
Serum creatinine: 1.2 mg/dL - down from 1.8
BUN: 11 - normalized from 42
The patient reported meaningful symptom improvement: reduced fatigue, improved mood, and greater overall energy. The nephrologist's recommendation had been watchful waiting. What the labs documented instead was a shift across a CKD staging threshold in the direction of recovery.
Discussion
The ECM is a rate-limiting factor in renal function. The extracellular matrix is not passive scaffolding. It is the functional medium through which all substances transit between the bloodstream and parenchymal cells. When the ECM is congested with homotoxins and metabolic waste - as Pischinger's ground regulation system and contemporary ECM research both describe - the transport function of the ground substance is impaired.
Nutrients, oxygen, and regulatory signals are delivered less efficiently. Metabolic waste is cleared more slowly. Renal tubular cells operating in a chronically congested matrix are under sustained biochemical stress independent of any structural kidney pathology. Drainage therapy, by supporting the emunctory organs and facilitating ECM clearance, addresses this rate-limiting factor directly.
Alkalinization and CKD. Metabolic acidosis is a recognized accelerant of CKD progression. It drives tubular ammonia production, activates complement, and promotes interstitial fibrosis. Sodium bicarbonate supplementation as a strategy to correct chronic metabolic acidosis in CKD has been studied in human clinical trials. Readers are directed to the work of de Brito-Ashurst et al. published in the Journal of the American Society of Nephrology (2009), which demonstrated slowed CKD progression and preserved muscle function in patients receiving bicarbonate supplementation. The naturopathic use of sodium bicarbonate for matrix alkalinization is mechanistically aligned with this evidence base.
The unaddressed root cause. The Entresto/NSAID combination represents an iatrogenic contributor to this patient's renal decline that was not identified or managed by his conventional care team. ARB-class medications and NSAIDs together reduce glomerular filtration pressure through complementary hemodynamic mechanisms. The naturopathic encounter was the first clinical context in which the patient's complete medication and OTC supplement picture was reviewed in the context of his renal trajectory. This is a core function of naturopathic medicine - and in this case, a gap in conventional management that had direct organ-level consequences.
Limitations. This is a single case report. Causation cannot be established. The multi-component nature of the protocol, the uncontrolled variable of ongoing nephrotoxic medication exposure, and the absence of a control condition all limit the strength of conclusions that can be drawn. What the case does establish is a clinically coherent, lab-documented trajectory of improvement in a patient whose conventional prognosis was progressive decline. That is sufficient justification for presenting it as a clinical observation worthy of attention.
Clinical Summary
A 73-year-old male with Stage 3b CKD, complex cardiovascular history, and longstanding polypharmacy achieved a documented GFR increase from 37 to 63 mL/min/1.73m² over approximately three months on a drainage-centered naturopathic protocol.
The primary interventions were the Hevert Detox Kit, GUNA drainage remedies targeting the ECM, lymph, liver and bowel, sodium bicarbonate for matrix alkalinization, and a trace mineral complex.
A nephrotoxic drug interaction (Entresto + NSAIDs) was identified retrospectively and represents a correctable conventional contributor to this patient's renal decline that had not been addressed.
Nettle seed tincture (Urtica dioica seed), used as a kidney trophorestorative at 20 drops twice daily in the subsequent treatment phase, was associated with consistent GFR recovery following episodic declines - a clinical pattern consistent with its traditional trophorestorative use, pending formal study.
In patients with declining GFR and complex pharmacological histories, terrain-based drainage therapy combined with medication review offers a clinically meaningful approach beyond watchful waiting.
Disclaimer: This article is for educational and informational purposes only and does not constitute medical advice. It describes a single clinical observation and should not be interpreted as a treatment protocol for chronic kidney disease or any other condition. All patients should remain under the active supervision of a licensed physician. The author does not assume liability for outcomes arising from the application of information contained herein.
Practitioners interested in European Biological Medicine drainage protocols are invited to explore the Foundations of European Drainage course at courses.drmarkiwanicki.com.
Potential clients interested in working together learn more about my online consults at https://drmarkiwanicki.com/work-with-me
References
Lapi F, Azoulay L, Yin H, Nessim SJ, Suissa S. Concurrent use of diuretics, angiotensin converting enzyme inhibitors, and angiotensin receptor blockers with non-steroidal anti-inflammatory drugs and risk of acute kidney injury: nested case-control study. BMJ. 2013;346:e8525. doi:10.1136/bmj.e8525
Harirforoosh S, Asghar W, Jamali F. Adverse effects of nonsteroidal antiinflammatory drugs: an update of gastrointestinal, cardiovascular and renal complications. J Pharm Pharm Sci. 2013;16(5):821-847. doi:10.18433/J3VW2F
Kraut JA, Madias NE. Metabolic acidosis of CKD: an update. Am J Kidney Dis. 2016;67(2):307-317. doi:10.1053/j.ajkd.2015.08.028
Goraya N, Wesson DE. Metabolic acidosis and the progression of chronic kidney disease. Curr Opin Nephrol Hypertens. 2016;25(3):193-198. doi:10.1097/MNH.0000000000000214
de Brito-Ashurst I, Varagunam M, Raftery MJ, Yaqoob MM. Bicarbonate supplementation slows progression of CKD and improves nutritional status. J Am Soc Nephrol. 2009;20(9):2075-2084. doi:10.1681/ASN.2008111205. PMID: 19608703
Winston D. Nettle seed (Urtica dioica) as a kidney trophorestorative. Cited in: Chrysalis Natural Medicine Clinic. Stinging Nettle (Urtica dioica). Available at: https://chrysalisnaturalmedicine.com/stinging-nettle-urtica-dioica/. Originally reported 1999.
Pischinger A. The Extracellular Matrix and Ground Regulation: Basis for a Holistic Biological Medicine. Edited by Hartmut Heine. Berkeley, CA: North Atlantic Books; 2007.